
Published on August 12, 2024
by Leor Sapir
Original: City Journal – A Consensus No Longer
The American Society of Plastic Surgeons becomes the first major medical association to challenge the consensus of medical groups over “gender-affirming care” for minors.
The main justification for “gender-affirming care” for minors in the United States has been that “all major U.S. medical associations” support it. Critics of this supposed consensus have argued that it is not grounded in high-quality research or decades of honest and robust deliberation among clinicians with different viewpoints and experiences. Instead, it is the result of a small number of ideologically driven doctor-association members in LGBT-focused committees, who exploit their colleagues’ trust. Physicians presenting different viewpoints are silenced or kept away from decision-making circles, ensuring the appearance of unanimity.
As the U.K.’s Cass Review pointed out, the World Professional Association for Transgender Health (WPATH) and the U.S. Endocrine Society were especially important in forging this consensus, and they did so by citing each other’s statements, rather than conducting a scientific appraisal of the evidence. The “circularity” of this approach, says Cass in her report to England’s National Health Service, “may explain why there has been an apparent consensus on key areas of practice despite the evidence being poor.”
Perhaps because it has never really depended on evidence, this doctor-group consensus has shown remarkable resilience in the face of major system shocks, including several whistleblowers, revelations from court documents that WPATH manipulated scientific evidence reviews, the Cass Review, a bipartisan commitment in the U.K. to roll back pediatric medical transition, and a growing international call for a developmentally informed approach that prioritizes psychotherapy over hormones and surgeries.
But the U.S. consensus now appears to have its first big fracture. In July, the American Society of Plastic Surgeons, a major medical association representing 11,000 members and over 90 percent of the field in the U.S. and Canada, told me that it “has not endorsed any organization’s practice recommendations for the treatment of adolescents with gender dysphoria.” ASPS acknowledged that there is “considerable uncertainty as to the long-term efficacy for the use of chest and genital surgical interventions” and that “the existing evidence base is viewed as low quality/low certainty.”
Calling the evidence for youth gender transition “low quality” is not, as some gender clinicians say, a “scary buzzword” intended to “confus[e] non-experts.” In evidence-based medicine, “low quality” evidence means something very specific: that the true effect of an intervention is likely to be markedly different from the results reported in studies. As one expert in evidence-based medicine put it, low quality “doesn’t just mean something esoteric about study design, it means there’s uncertainty about whether the long-term benefits outweigh the harms.” As evidence for those harms—which include infertility, sexual dysfunction, and the agony of regret—continues to mount and ethical concerns get harder to ignore, European countries are increasingly prioritizing psychotherapy and reclassifying endocrine and surgical approaches as experimental.
Aware that WPATH suppressed systematic reviews of evidence while developing its latest “standards of care,” ASPS says that it “is reviewing and prioritizing several initiatives that best support evidence-based gender surgical care to provide guidance to plastic surgeons.” I also asked ASPS whether plastic surgeons share responsibility for determining the medical necessity of gender surgeries for minors. ASPS responded that surgeons are “members of the multidisciplinary care team” and as such “have a responsibility to provide comprehensive patient education and maintain a robust and evidence-based informed consent process, so patients and their families can set realistic expectations in the shared decision-making process.”
Sheila Nazarian, a plastic surgeon who practices in Beverly Hills, California, told me that colleagues in her field are increasingly expressing concern about the use of hormones and surgeries to help minors who experience distress associated with their sex. Many, however, fear that voicing these concerns will bring professional and social blowback. “It’s a real problem when colleagues are afraid to debate any medical treatment or procedure, and especially when minors are the patients,” Nazarian says. “I have been following the international debate on youth gender medicine for some time now and know we [in the U.S.] are far behind in recognizing the lack of evidence for long-term benefits, something that our European colleagues have done.”
One obstacle to having productive discussions, Nazarian said, is the partisan divide over youth gender medicine, which leads physicians to believe that disagreement with the “gender-affirming” approach is driven by political or ideological considerations. This perception is understandable, given that the debate is in fact polarized along partisan lines, though it has become less so in the last two years as a number of Democrats in state legislatures have voted in favor of (or abstained from voting against) age restriction laws. It’s possible that advocates of “gender-affirming” interventions see benefit in the partisan framing, as it may deter liberal doctors from examining the issue in greater depth and speaking up when they detect problems.
Regardless of why the issue is polarized in the U.S., the growing international consensus against the “gender affirming” approach for minors is anything but partisan. In Finland and Sweden, for instance, left-leaning governments implemented restrictions following systematic reviews of evidence by independent health-care quality agencies. In the U.K., the NHS-commissioned independent review of the Gender Identity Development Service, led by Hilary Cass, prompted the Tory government to ban puberty blockers, a move subsequently endorsed by the new Labour government.
The U.S. is one of the few Western countries where minors can receive gender surgeries, according to a new report. Teens under 18 cannot undergo double mastectomy in Belgium, Finland, Germany, Luxemburg, Sweden, the U.K., and three Canadian provinces. Countries that allow these procedures typically do so only in “rare cases,” after age 16, and with parental consent. In the U.S., WPATH Standards of Care, Version 8, widely followed and endorsed by the Biden administration, specifies no age minimums for gender surgeries, with the exception of phalloplasty (but even that can be performed if “significant, compelling reasons” exist to do so). In June, unsealed court documents revealed that WPATH eliminated age minimums for political reasons, and under pressure from U.S. Assistant Secretary for Health Rachel Levine, a transgender woman.
An estimate of U.S. “gender-affirming” double mastectomies published in 2023 in the Journal of the American Medical Association reported 3,125 cases of “breast or chest procedures” in patients ages 12 to 18 between 2016 to 2020. The study did not differentiate between 18-year-olds and minors. A new analysis by the Manhattan Institute, using a more up-to-date all-payer national insurance database from 2017 to 2023, found evidence of 5,288 to 6,294 “gender-affirming” double mastectomies for girls under age 18. This includes 50 to 179 girls who were 12.5 or younger at the time of their procedure. (“Top surgery” on 12-year-old girls has been reported in the medical literature.)
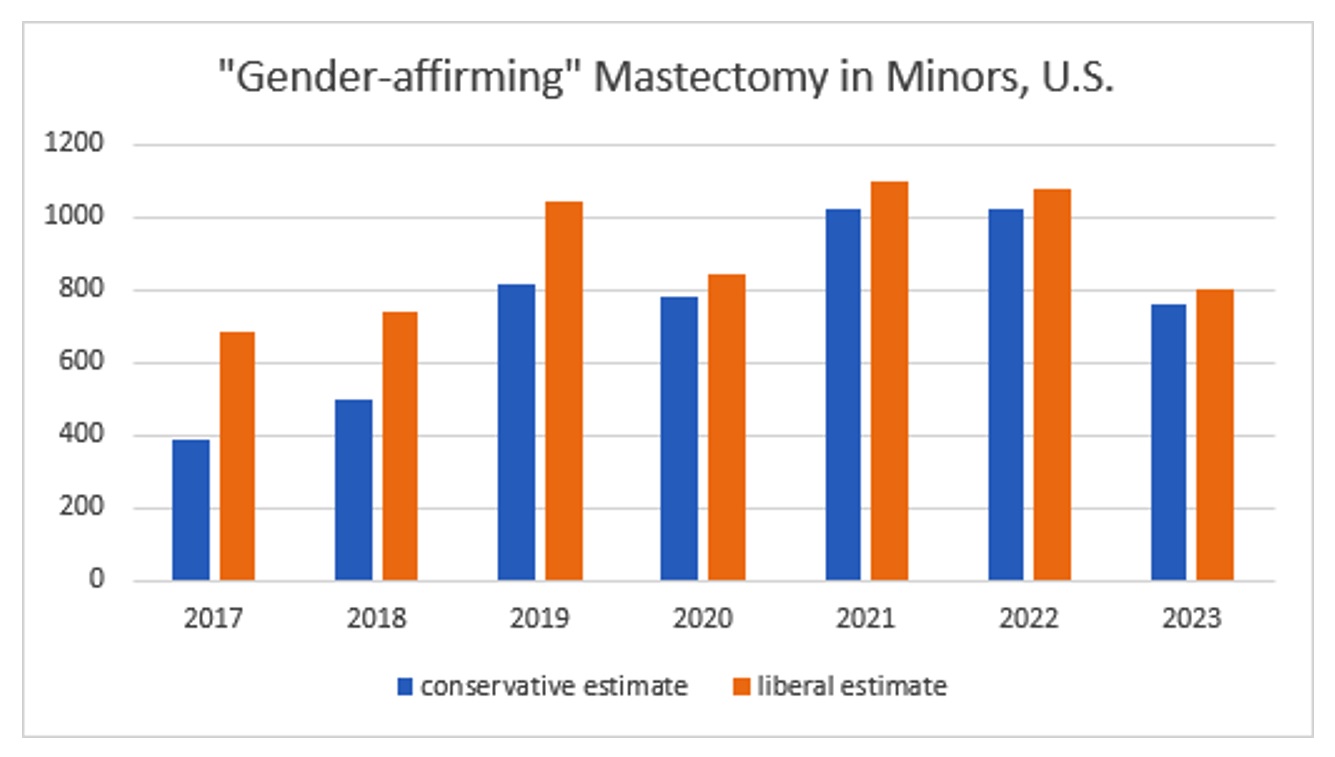
Source: all-payer all claims database, acquired by Manhattan Institute
Two caveats should be mentioned. First, 2023 data are incomplete, making it premature to conclude that a dip occurred that year, relative to previous years. Second, even the liberal estimates are an undercount, as the data are limited by two constraints: the procedures had to be covered by insurance, and patients had to have a preexisting diagnosis of gender dysphoria. The out-of-pocket costs of “top surgery” can be as low as $3,000, a sum many middle-class families can afford. Further, if it is true, as is being alleged, that gender clinicians are using false diagnostic and procedural codes for insurance billing, these cases would not show up in our data.
A growing trend in gender medicine is “nonbinary” mastectomies, a procedure that some patients seek in order to appear neither male nor female. According to our data, a minimum of 1,873 such procedures (conservative estimate) were performed on girls under age 18 in the U.S. between 2017 and 2023. The number of procedures grew from 70 in 2017 to 470 in 2023—an almost seven-fold rise. Plastic surgeons who perform these procedures leverage the existing billing code for breast reduction (“19318–Unilateral reduction mammaplasty”), a practice some might argue amounts to insurance fraud.
When speaking to the public, American gender clinicians have a tendency vastly to understate or even deny the existence of gender surgeries on minors. For example, in 2023, Marci Bowers, a plastic surgeon and president of WPATH, told CBS News that “Surgery really is not done under the age of 18, except in severe cases . . . And even that is rare, I think the estimates are something like 57 surgeries under the age of 18 were done for trans individuals.” (Bowers, a genital surgery specialist, may have been thinking about genital surgery on minors, of which at least 56 were performed between 2019 and 2021, according to a Reuters report.)
At an April 2023 hearing before the Texas Senate Committee on Health and Human Services, Cody Miller Pyke, a physician and gender medicine advocate, said that “children under the age of eighteen in this country do not have gender reassignment surgery. There isn’t a single case.” Texas Pediatric Society president Louis Appel testified that “surgeries are not part of the standard of care.” This was seven months after WPATH published its Standards of Care, Version 8, which includes gender surgeries with no age minimums.
Due to the nature of their work, plastic surgeons are increasingly finding themselves in the hot seat of gender medicine lawsuits. Almost two dozen lawsuits by detransitioners against clinics and clinicians are currently underway, and at least seven of the defendants in these cases are ASPS members. One, Winnie Tong, performed a double mastectomy on Kayla Lovdahl in 2017, when she was only 13. Lovdahl is now suing Kaiser Permanente and Tong, who claim that they were following WPATH’s Standards of Care, Version 7—a guideline so poor in its quality that it does not meet Kaiser’s own explicitly stated criteria for what makes a clinical guideline trustworthy.
Whether detransitioners like Lovdahl will win in court depends largely on how the courts understand the standard of care—a medical-legal term—at the time defendants performed the surgeries. WPATH calls its recommendations “standards of care,” likely because it recognizes—or hopes—that judges will look to these recommendations when determining what the standard of care was and whether the defendants deviated from it. But the unsealed court documents from the lawsuit challenging Alabama’s age restriction law revealed that WPATH wrote its current standards of care explicitly with a view to eventual litigation, even consulting an ACLU lawyer in the process. The ACLU has regularly cited WPATH’s standards of care in its legal briefings to argue that its legal position is grounded in medical science—a claim that seems, at the least, to represent circular reasoning.
If surgeons who perform double mastectomy or vaginoplasty on teenagers lose in court, the judgment will show up on their board of medicine examiner website and on their license. Malpractice premiums in this area are already rising, and some insurers outright exclude under-18 gender-transition procedures from their coverage policies. California, where Chloe Cole and Kayla Lovdahl are suing Kaiser Permanente, limits punitive damages to nine times the total amount of special and general damages awarded. This could bring the total awarded to each plaintiff to as high as $18 million, according to an attorney familiar with the case.
Kevin Keller, a lawyer who specializes in health-care-related tort litigation, told me that medical malpractice is actually the lesser worry for clinicians here. Plaintiffs can also allege “intentional acts,” a category of behaviors including fraud that are typically excluded under medical malpractice insurance policies. In her lawsuit against Eric T. Emerson—an ASPS member—and his clinic, Piedmont Plastic Surgery and Dermatology in North Carolina, Prisha Mosley, a former patient, alleges that Emerson “misled and deceived [her] into thinking that surgery on her healthy breasts would benefit her and that she needed this surgery.” Juries can award massive damages for such tort claims, and these will be borne directly by the surgeon and the clinic. “Juries can easily award plaintiffs like Mosley $10 million or more,” Keller said. “And that’s money that doctors and clinics will have to pay out of pocket.”
A key question for these lawsuits is the degree to which surgeons are responsible for determining the medical necessity of the procedures that they are asked to perform. According to Mosley’s complaint, for instance, Emerson, the surgeon, “noted” her “history of anxiety and anorexia nervosa and family history of depression” but did not see any of these issues as red flags and did not “form an evidence-based, independent judgment” about the medical necessity of mastectomy in her case.
Existing guidelines like the ones issued by WPATH and the Endocrine Society envision surgeons as part of a “multidisciplinary” team that includes mental-health professionals. Though WPATH recommends that surgeons have special training in “gender-affirming care,” it is unclear whether surgeons can second-guess the appropriateness of surgery (except if there are physical contraindications) once a patient has been “affirmed” and given the all-clear by a mental-health professional. Doing so would constitute “gatekeeping,” which is seen in the gender medicine community as “non-affirming” and harmful. “Treatment” is oriented around “the child’s sense of reality and feeling of who they are,” says Jason Rafferty, who wrote the American Academy of Pediatrics’ statement on “gender-affirming care” at the very beginning of his medical career and who is now being sued by two former patients.
Kayla Lovdahl, the young woman currently suing Kaiser Permanente, was approved for surgery after an “affirming” psychologist conducted a single 75-minute evaluation and determined that she was “transgender,” according to her legal complaint. Five weeks later, Lovdahl, still only 12, met with the plastic surgeon, Winnie Tong, who concluded after a 30-minute evaluation that she fulfilled criteria for a double mastectomy. The procedure was performed four months later, just after Lovdahl turned 13.
In July, the Pennsylvania Psychological Association, a branch of the American Psychological Association, forbade any mention of the Cass Review on its professional listserv. Doing so, the leadership suggested, could cause “harm” to colleagues with “very different points of view based on their varied life experiences.” This is but one of many examples of how the mental health profession has abdicated its role in ensuring that young people with mental health challenges are provided evidence-based care. It is likely a matter of time before judges come to appreciate how this area of medicine operates and refuse to let surgeons off the hook when they assert that they were relying on mental health professionals to determine medical necessity.
Gender clinics across the country have adopted letter-of-support and letter-of-medical-necessity templates to ensure that adolescents seeking surgery get approval, with few hiccups. The message these templates implicitly send to therapists, who are the first and arguably most important gatekeepers, is that gender surgery for minors is a standard procedure rather than an extreme departure requiring strong evidence.
The gender clinic at Seattle Children’s Hospital is an example of a major clinic that offers mental-health professionals a template to use for writing letters of support for surgery. The template contains language designed to bypass any concern that the candidate fits the profile of “rapid onset gender dysphoria” (ROGD), the most common adolescent presentation and the one that prompted the course reversal in Europe. The template effectively instructs the referring therapist to attest that the ROGD presentation is really just a teen who has always known he or she was transgender but only disclosed that information to his or her parents during adolescence. This common anti-ROGD refrain is based on highly dubious research.
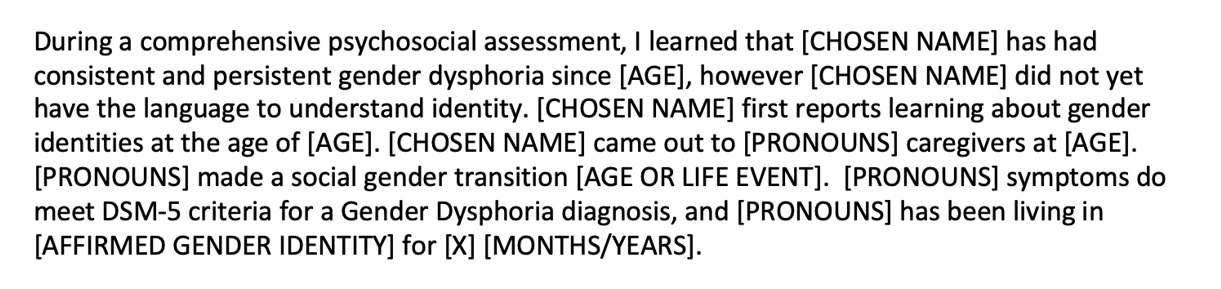
Source: Gender Clinic, Seattle Children’s Hospital
Nazarian, the Beverly Hills surgeon, told me that surgeons in her professional network who perform gender surgeries typically defer to mental-health professionals and endocrinologists to determine for them whether minors should receive procedures like double mastectomy. That approach, she believes, is misguided, and reduces surgeons to mechanics.
“We are not highly trained technicians,” Nazarian told me. “We are physicians with responsibility for the health and well-being of our patients. We can get input from other clinicians, but ultimately the responsibility for determining medical readiness lies with us. That means that we have to examine all the data and studies available to us. Furthermore, you can’t help people by ignoring the reasons they want to go under the knife. With every patient, I exercise discretion as a professional and determine whether the procedure they are seeking is in their ultimate best interest.” The idea that surgeons should defer heavily to the prior assessments of clinicians struck Nazarian as wrong. “You can’t outsource your professional judgement to other clinicians. It’s your responsibility as the last in a chain of treatment to ensure you are doing what is best for the patient now and in the long term.”